Muscular System
Article objectives
The muscular system is the biological system of humans that allows them to move. The muscular system, in vertebrates, is controlled through the nervous system. Much of your muscle movement occurs without your conscious control and is necessary for your survival. The contraction of your heart and peristalsis, the intestinal movements that pushes food through your digestive system, are examples of involuntary muscle movements. Involuntary muscle movement is controlled by the autonomic nervous system. Voluntary muscle contraction is used to move the body and can be finely controlled, such as the pincer-type movement of the fingers that is needed to pick up chess pieces, or the gross movements of legs arm, and the torso that are needed in skating, shown in Figure 1. Voluntary muscle movement is controlled by the somatic nervous system.

Figure 1: You need muscles to play chess. Playing chess requires fine motor movement, but not a lot of gross muscle movements. Skating on the other hand, requires a lot of gross muscle movement of the limbs and the entire body.
Muscle Tissues
Each muscle in the body is composed of specialized structures called muscle fibers. Muscle fibers are long, thin cells that have a special talent that other cells do not have—they are able to contract. Muscles, where attached to bones or internal organs and blood vessels, are responsible for movement. Nearly all movement in the body is the result of muscle contraction. Exceptions to this are the action of cilia, the flagellum on sperm cells, and the amoeboid movement of some white blood cells.
Three types of muscle tissue are in the body: skeletal, smooth, and cardiac.
• Skeletal muscle is usually attached to the skeleton. Skeletal muscles are used to move the body. They generally contract voluntarily (controlled by the somatic nervous system), although they can also contract involuntarily through reflexes.
• Smooth muscle is found within the walls of organs and structures such as the esophagus, stomach, intestines, bronchi, uterus, urethra, bladder, and blood vessels. Unlike skeletal muscle, smooth muscle is involuntary muscle which means it not under your conscious control.
• Cardiac muscle is also an involuntary muscle but is a specialized kind of muscle found only within the heart.
Cardiac and skeletal muscles are striated, in that they contain highly-regular arrangements of bundles of protein fibers that give them a “striped” appearance. Smooth muscle does not have such bundles of fibers, and is non-striated. While skeletal muscles are arranged in regular, parallel bundles, cardiac muscle fibers connect at branching, irregular angles. Skeletal muscle contracts and relaxes in short, intense bursts, whereas cardiac muscle contracts constantly for 70 to 80 years (an average life span), or even longer.
Skeletal Muscle
Skeletal muscle, which is attached to bone, is responsible for body movements and body posture. There are approximately 639 skeletal muscles in the human body, some of which are shown in Figure 2. These muscles are under conscious, or voluntary, control. The basic units of skeletal muscle are muscle cells that have many nuclei. These muscle cells also contain light and dark stripes called striations, which are shown in Figure 2. The striations are a result of the orientation of the contractile proteins inside the cells. Skeletal muscle is therefore called striated muscle. Each muscle cell acts independently of its neighboring muscle cells. On average, adult males are made up of 40 to 50 percent skeletal muscle tissue and an adult female is made up of 30 to 40 percent skeletal muscle tissue.
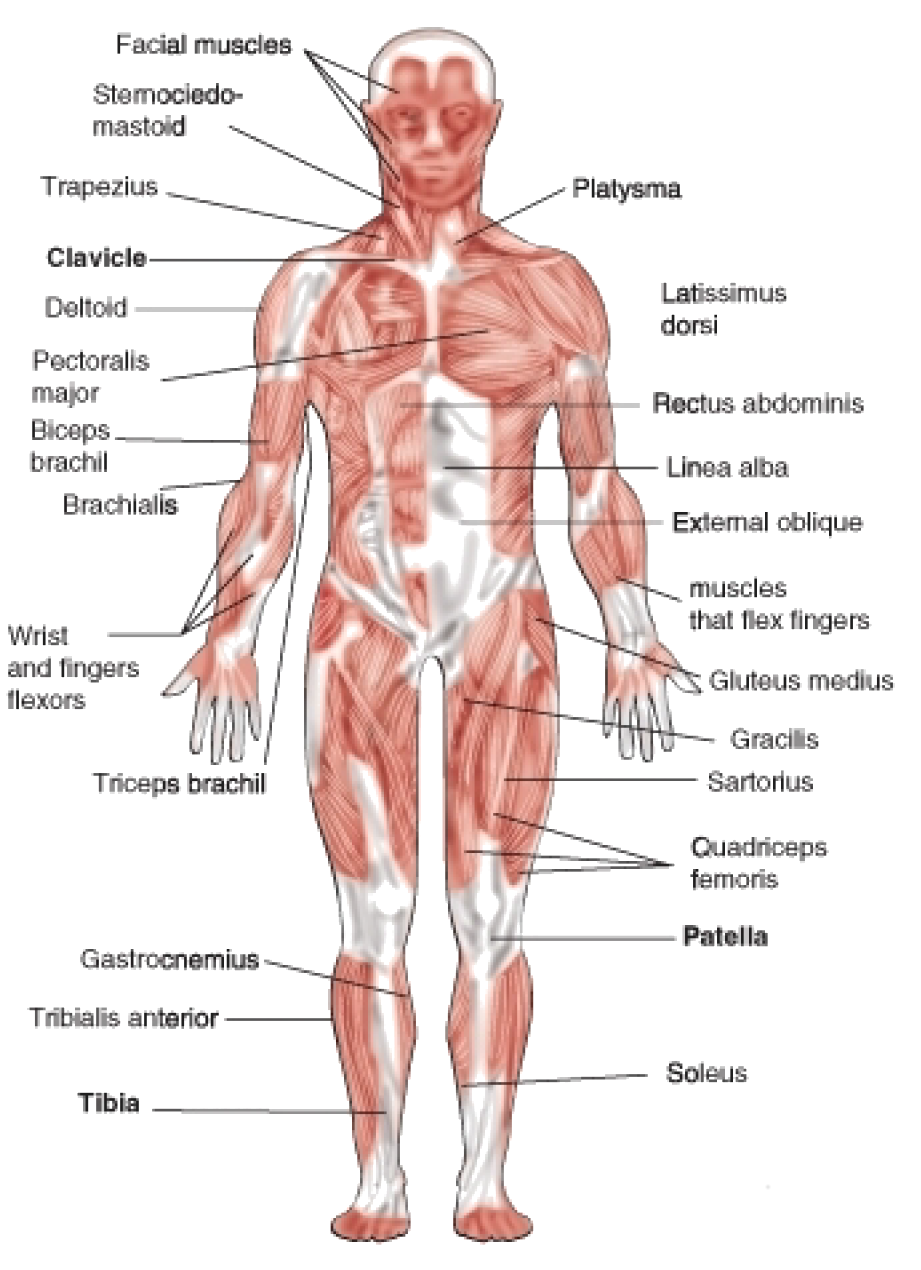
Figure 2: Frontal view of the major skeletal muscles. You would not see smooth and cardiac muscles included in diagrams of the muscular system because such diagrams usually show only the muscles that move the body (skeletal muscles).

Figure 3: Micrograph of skeletal muscle. The stripy appearance of skeletal muscle tissue is due to long protein filaments that run the length of the fibers.
Smooth Muscle
Smooth muscle is found in the walls of the hollow internal organs such as blood vessels, the intestinal tract, urinary bladder, and uterus. It is under control of the autonomic nervous system. This means that smooth muscle cannot be controlled consciously, so it is also called involuntarily muscle. Smooth muscle cells do not have striations, and so smooth muscle is also called non-striated muscle. Smooth muscle cells are spindle-shaped and have one central nucleus. The cells are generally arranged in sheets or bundles, rather than the regular grouping that skeletal muscle cells form, and they are connected by gap junctions. Gap junctions are little pores or gaps in the cell membrane that link adjoining cells and they allowing quick passage of chemical messages between cells. Smooth muscle is very different from skeletal muscle and cardiac muscle in terms of structure and function, as shown in Figure 4. Smooth muscle contracts slowly and rhythmically.

Figure 4: Smooth muscle. The appearance of smooth muscle is very different from skeletal and cardiac muscle. The muscle protein fibers within smooth muscle are arranged very differently to the protein fibers of skeletal or cardiac fibers, shown in (a). The spindly shape of smooth muscle cells can be seen in (b).
Cardiac Muscle
Cardiac muscle, which is found in the walls of the heart, is under control of the autonomic nervous system, and so it is an involuntary muscle. A cardiac muscle cell has characteristics of both a smooth muscle and skeletal muscle cell. It has one central nucleus, similar to smooth muscle, but it striated, similar to skeletal muscle. The cardiac muscle cell is rectangular in shape, as can been seen in Figure 5. The contraction of cardiac muscle is involuntary, strong, and rhythmical. Cardiac muscle has many adaptations that makes it highly resistant to fatigue. For example, it has the largest number of mitochondria per cell of any muscle type. The mitochondria supply the cardiac cells with energy for constant movement. Cardiac cells also contain myoglobins (oxygen-storing pigments), and are provided with a large amount of nutrients and oxygen by a rich blood supply.

Figure 5: Cardiac muscle. Cardiac muscle fibers are connected together through intercalated discs.
Cardiac muscle is similar to skeletal muscle in chemical composition and action. However, the structure of cardiac muscle is different in that the muscle fibers are typically branched like a tree branch, and connect to other cardiac muscle fibers through intercalcated discs, which are a type of gap junction. A close-up of an intercalated disc is shown in Figure 5. Cardiac muscle fibers have only one nucleus.
Structure of Muscle Tissue
A whole skeletal muscle is an organ of the muscular system. Each skeletal muscle consists of skeletal muscle tissue, connective tissue, nerve tissue, and vascular tissue. Skeletal muscles vary considerably in size, shape, and arrangement of fibers. They range from extremely tiny strands such as the tiny muscles of the middle ear to large masses such as the quadriceps muscles of the thigh.
Each skeletal muscle fiber is a single large, cylindrical muscle cell. Skeletal muscle fibers differ from “regular” body cells. They are multinucleated, which means they have many nuclei in a single cell; during development many stem cells called myoblasts fuse together to form muscle fibers. Each nucleus in a fiber originated from a single myoblast. Smooth and cardiac muscle fibers do not develop in this way.
An individual skeletal muscle may be made up of hundreds, or even thousands, of muscle fibers that are bundled together and wrapped in a connective tissue covering called epimysium. Fascia, connective tissue outside the epimysium, surrounds and separates the skeletal muscles. Portions of the epimysium fold inward to divide the muscle into compartments called fascicles. Each fascicle compartment contains a bundle of muscle fibers, as shown in Figure 6.

Figure 6: Individual bundles of muscle fibers are called fascicles. The cell membrane surrounding each muscle fiber is called the sarcolemma, and beneath the sarcolemma lies the sarcoplasm, which contains the cellular proteins, organelles, and myofibrils. The myofibrils are composed of two major types of protein filaments: the thinner actin filament, and the thicker myosin filament. The arrangement of these two protein filaments gives skeletal muscle its striated appearance.
Skeletal muscle fibers, like body cells, are soft and fragile. The connective tissue covering give support and protection for the delicate cells and allow them to withstand the forces of contraction. The coverings also provide pathways for the passage of blood vessels and nerves. Active skeletal muscle needs efficient delivery of nutrients and oxygen, and removal of waste products, both of which are carried out by a rich supply of blood vessels.
Muscles and Bones
Muscles move the body by contracting against the skeleton. Muscles can only actively contract, they extend (or relax) passively. The ability of muscles to move parts of the body in opposite directions requires that they be attached to bones in pairs which work against each other (called antagonistic pairs). Generally, muscles are attached to one end of a bone, span a joint, and are attached to a point on the other bone of the joint. Commonly, the connective tissue that covers the muscle extends beyond the muscle to form a thick rope-like structure called a tendon, as shown in Figure 6. One attachment of the muscle, the origin, is on a bone that does not move when the muscle contracts. The other attachment point, the insertion, is on the bone that moves. Tendons and muscles work together and exert only a pulling force on joints.

Figure 7: Movement of the elbow joint involves muscles and bones. The contraction of the biceps brachii muscle pulls on the radius, its point of insertion, which causes the arm to bend. To straighten the arm, the triceps brachii muscle contracts and pulls on the ulna, this causes the arm to straighten.
For example, when you contract your biceps brachii muscles, shown in Figure 7, the force from the muscles pulls on the radius bone (its point of insertion) causing the arm to move up. This action decreases the angle at the elbow joint (flexion). Flexion of the elbow joint is shown in Figure 8. A muscle that causes the angle of a joint to become smaller is called a flexor. To extend, or straighten the arm, the biceps brachii relaxes and the triceps on the opposite side of the elbow joint contracts. This action is called extension, and a muscle that causes a joint to straighten out is called an extensor. In this way the joints of your body act like levers that reduce the amount of effort you have to expend to cause large movements of the body.

Figure 8: (a) The position of the biceps brachii. (b) The biceps brachii and triceps brachii act as an atagonistic pair of muscles that move the arm at the elbow joint. The biceps muscle is the flexor, and the triceps, at the back of the arm, is the extensor (c).
Muscle Contractions
A muscle contraction occurs when a muscle fiber generates tension through the movement of actin and myosin. Although you might think the term contraction means only ”shortening,” the overall length of a contracted muscle may stay the same, or increase, depending on the force working against the muscle.

Figure 9: The components of muscle contraction. The sacromere is the functional unit of muscle contraction; it reaches from one Z-line to the next (also shown in Figure 10). In a relaxed muscle, the actin (thin filament) and myosin (thick filament) overlap. In a muscle contraction, the filaments slide past each other, shortening the sacromere. This model of contraction is called the sliding filament mechanism.
Each muscle fiber contains cellular proteins and hundreds or thousands of myofibrils. Each myofibril is a long, cylindrical organelle that is made up of two types of protein filaments: actin and myosin. The actin filament is thin and threadlike, the myosin filament is thicker. Myosin has a “head” region that uses energy from ATP to “walk” along the actin thin filament (Figure 12). The overlapping arrangement of actin and myosin filaments gives skeletal muscle its striated appearance. The actin and myosin filaments are organized into repeating units called sarcomeres, which can be seen in Figure 9. The thin actin filaments are anchored to structures called Z lines. The region from one Z line to the next makes up one sacromere. When each end of the myosin thick filament moves along the actin filament, the two actin filaments at opposite sides of the sacromere are drawn closer together and the sarcomere shortens, as shown in Figure 10. When a muscle fiber contracts, all sarcomeres contract at the same time, which pulls on the fiber ends.

Figure 10: When each end of the myosin thick filament moves along the actin filament, the two actin filaments at opposite sides of the sacromere are drawn closer together and the sarcomere shortens.
The Neuromuscular Junction
For skeletal (voluntary) muscles, contraction occurs as a result of conscious effort that comes from the brain. The brain sends nerve signals, in the form of action potentials to the motor neuron that innervates the muscle fiber, such as the motor neuron in Figure 12. In the case of some reflexes, the signal to contract can originate in the spinal cord through a reflex arc. Involuntary muscles such as the heart or smooth muscles in the gut and vascular system contract as a result of non-conscious brain activity or stimuli endogenous to the muscle itself. Other actions such as body motion, breathing, and chewing have a reflex aspect to them; the contractions can be initiated consciously or unconsciously, but are continued through unconscious reflexes.

Figure 11: (a) A simplified diagram of the relationship between a skeletal muscle fiber and a motor neuron at a neuromuscular junction. 1. Axon; 2. Synaptical junction; 3. Muscle fiber; 4. Myofibril. (b) A close-up view of a neuromuscular junction. The neurotransmitter acetylcholine is released into the synapse and binds to receptors on the muscle cell membrane. The acetylcholine is then broken down by enzymes in the synapse. 1. presynaptic terminal; 2. sarcolemma; 3. synaptic vesicles; 4. Acetylcholine receptors; 5. mitochondrion.
The Sliding Filament Theory
The widely accepted theory of how muscles contract is called the sliding-filament model (also known as the sliding filament theory), which is shown in Figure 12. The presence of calcium ions (\(Ca^{2+}\)) allows for the interaction of actin and myosin. In the resting state, these proteins are prevented from coming into contact. Two other proteins, troponin and tropomyosin, act as a barrier between the actin and myosin, preventing contact between them. When \(Ca^{2+}\) binds to the actin filament, the shape of the troponin-tropomyosin complex changes, allowing actin and myosin to come into contact with each other. Below is an outline of the sliding filament theory.

Figure 12: The process of actin and myosin sliding past one another is called crossbridge cycling, and it occurs in all muscle types. Myosin is a molecular motor that moves along the passive actin. Each thick myosin filament has little extensions or “heads,” that “walk” along the thin actin filaments during contraction. In this way the thick filament slides over thin filament. The actin filaments transmit the force generated by myosin to the ends of the muscle, which causes the muscle to shorten.
- An action potential arrives at the axon terminal of a motor neuron.
- The arrival of the action potential activates voltage-dependent calcium channels at the axon terminal, and calcium rushes into the neuron.
- Calcium causes vesicles containing the neurotransmitter acetylcholine to fuse with the plasma membrane, which releases acetylcholine into the synaptic cleft between the axon terminal and the motor end plate of the skeletal muscle fiber.
- Activation of the acetylcholine receptors on the muscle fiber membrane opens its sodium/potassium channel, which triggers an action potential in the muscle fiber.
- The action potential spreads through the muscle fiber’s network, depolarizing the inner portion of the muscle fiber.
- The depolarization activates specialized storage sites throughout the muscle, called the sarcoplasmic reticulum, to release calcium ions (\(Ca^{++}\)). The sarcoplasmic reticulum is a special type of smooth endoplasmic reticulum found in smooth and skeletal muscle that contains large amounts of \(Ca^{++}\), which it stores and then releases when the cell is depolarized.
- The calcium ions bind to actin filaments of the myofibrils and activate the actin for attachment by the myosin heads filaments.
- Activated myosin binds strongly to the actin filament. Upon strong binding, myosin rotates at the myosin-actin interface which bends a region in the “neck” of the myosin “head,” as shown in Figure 12.
- Shortening of the muscle fiber occurs when the bending neck of the myosin region pulls the actin and myosin filaments across each other. Meanwhile, the myosin heads remain attached to the actin filament, as shown in Figure 12.
- The binding of adenosine triphosphate (ATP) allows the myosin heads to detach from actin. While detached, ATP breaks down to adenosine diphosphate and an inorganic phosphate (ADP + Pi). The breaking of the chemical bond in ATP gives energy to the myosin head, allowing it to bind to actin again.
- Steps 9 and 10 repeat as long as ATP is available and \(Ca^{++}\) is present on the actin filament. The collective bending of numerous myosin heads (all in the same direction) moves the actin filament relative to the myosin filament which causes a shortening of the sacromere. Overall, this process results in muscle contraction. The sarcoplasmic reticulum actively pumps \(Ca^{++}\) back into itself. Muscle contraction stops when \(Ca^{++}\) is removed from the immediate environment of the myofilaments.
Motor Units
It is important to remember that the sliding filament theory applies to groups of individual muscle fibers which, along with their motor neuron, are called motor units. A single, momentary contraction is called a muscle twitch. A twitch is the response to a single stimulus that can involve a number of motor units. As a stimulus increases, more motor units are stimulated to contract until a maximum level is reached at which point the muscle cannot exert any more force.
Each muscle fiber contracts on an ”all or nothing” principle, a muscle fiber either contracts fully, or not at all, and all the fibers in a single motor unit contract at the same time. When a muscle is required to contract during exercise not all motor units are contracted at the same time. Most movements require only a small amount of the total force possible by the contraction of an entire muscle. As a result, our nervous system grades the intensity of muscle contraction by using different numbers of motor units at a time.
Cardiac Muscle Contractions
Cardiac muscle is adapted to be highly resistant to fatigue: it has a large number of mitochondria which allow continuous aerobic respiration; numerous myoglobins (oxygen storing pigment); and a good blood supply, which provides nutrients and oxygen. The heart is so tuned to aerobic metabolism that it is unable to pump well when there is a lack of blood to the heart muscle tissue, which can lead to a heart attack.
Unlike skeletal muscle, which contracts in response to nerve stimulation, and like certain types of smooth muscle, cardiac muscle is able to initiate contraction by itself. As a result, the heart can still beat properly even if its connections to the central nervous system are completely severed. A single cardiac muscle cell, if left without input, will contract rhythmically at a steady rate; if two cardiac muscle cells are in contact, whichever one contracts first will stimulate the other to contract, and so on. This inherent ability to contract is controlled by the autonomic nervous system.
If the rhythm of cardiac muscle contractions is disrupted for any reason (for example, in a heart attack or a cardiac arrest), erratic contractions called fibrillation can result. Fibrillation, which is life threatening, can be stopped by use of a device called a defibrillator. Defibrillation consists of delivering a therapeutic dose of electrical energy to the heart which depolarizes part of the heart muscle. The depolarization stops the fibrillation, and allows a normal heartbeat to start up again. Most types of defibrillators are operated by medical personnel only. However, you may be familiar with an automated external defibrillator (AED) which is shown in Figure 13.

Figure 13: A wall-mounted automated external defibrillator (AED). Defibrillators are used to “shock” fibrillating cardiac muscle back into the correct rhythm. AEDs are designed to be able to diagnose fibrillation in a person who has collapsed, meaning that a bystander can use them successfully with little or no training. They are usually found in areas where large groups of people may gather, such as train stations, airports, or at sports events.
Smooth Muscle Contraction
Smooth muscle-containing tissue, such as the stomach or urinary bladder often must be stretched, so elasticity is an important characteristic of smooth muscle. Smooth muscle (like cardiac muscle) does not depend on motor neurons to be stimulated. However, motor neurons of the autonomic nervous system do reach smooth muscle, causing it to contract or relax, depending on the type of neurotransmitter that is released. Smooth muscle is also affected by hormones. For example, the hormone oxytocin causes contraction of the uterus during childbirth.
Similar to the other muscle types, smooth muscle contraction is caused by the sliding of myosin and actin filaments over each other. However, calcium initiates contractions in a different way in smooth muscle than in skeletal muscle. Smooth muscle may contract phasically with rapid contraction and relaxation, or tonically with slow and sustained contraction. The reproductive, digestive, respiratory, and urinary tracts, skin, eye, and vasculature all contain smooth muscle. For example, the ability of vascular smooth muscle (veins and arteries) to contract and dilate is critical to the regulation of blood pressure. Smooth muscle contracts slowly and may maintain the contraction (tonically) for prolonged periods in blood vessels, bronchioles, and some sphincters. In the digestive tract, smooth muscle contracts in a rhythmic peristaltic fashion. It rhythmically massages products through the digestive tract, shown in Figure 14, as the result of phasic contraction.

Figure 14: The intestinal tract contains smooth muscle which moves food along by contracting and relaxing in a process called peristalsis.
Energy Supply for Muscle Contraction
Energy for the release and movement of the myosin head along the actin filament comes from ATP. The role of ATP in muscle contraction can be observed in the action of muscles after death, at which point ATP production stops. Without ATP, myosin heads are unable to release from the actin filaments, and remain tightly bound to it (a protein complex called actomyosin). As a result, all the muscles in the body become rigid and are unable to move, a state known as rigor mortis. Eventually, enzymes stored in cells are released, and break down the actomyosin complex and the muscles become ”soft” again.
Cellular respiration is the process by which cells make ATP by breaking down organic compounds from food. Muscle cells are able to produce ATP with oxygen which is called aerobic respiration, or without oxygen, an anaerobic process called anaerobic glycolysis or fermentation. The process in which ATP is made is dependent on the availability of oxygen.
Aerobic ATP Production
During everyday activities and light exercise, the mitochondria of muscle fibers produce ATP in a process called aerobic respiration. Aerobic respiration requires the presence of oxygen to break down food energy (usually glucose and fat) to generate ATP for muscle contraction. Aerobic respiration produces large amounts of ATP, and is an efficient means of making ATP. Up to 38 ATP molecules can be made for every glucose molecule that is broken down. It is the preferred method of ATP production by body cells. Aerobic respiration requires large amount of oxygen, and can be carried out over long periods of time. As activity levels increase, breathing rate increases to supply more oxygen for increased ATP production.
Anaerobic ATP Production
When muscles are contracting very quickly, which happens during vigorous exercise, oxygen cannot travel to the muscle cells fast enough to keep up with the muscles’ need for ATP. At this point, muscle fibers can switch to a breakdown process that does not require oxygen. The process, called anaerobic gylcolysis (sometimes called anaerobic respiration) breaks down energy stores in the absence of oxygen to produce ATP.
Anaerobic glycolysis produces only two molecules of ATP for every molecule of glucose, so it a less efficient process than aerobic metabolism. However, anaerobic glycolysis produces ATP about 2.5 times faster than aerobic respiration does. When large amounts of ATP are needed for short periods of vigorous activity, glycolysis can provide most of the ATP that is needed. Anaerobic glycolysis also uses up a large amount of glucose to make relatively small amounts of ATP. In addition to ATP, large amounts of lactic acid are also produced by glycolysis. When lactic acid builds up faster than it can be removed from the muscle, it can lead to muscle fatigue. Anaerobic glycolysis can be carried out for only about 30 to 60 seconds. Some recent studies have found evidence that mitochondria inside the muscle fibers are able to break down lactic acid (or lactate) to produce ATP, and that endurance training results in more lactate being is taken up by mitochondria to produce ATP.
Functions of Skeletal Muscle Contraction
In addition to movement, skeletal muscle contraction also fulfills three other important functions in the body: posture, joint stability, and heat production.
• Joint stability refers to the support offered by various muscles and related tissues that surround a joint.
• Heat production by muscle tissue makes them an important part of the thermoregulatory mechanism of the body. Only about 40 percent of energy input from ATP converts into muscular work, the rest of the energy is converted to thermal energy (heat). For example, you shiver when you are cold because the moving (shivering) skeletal muscles generate heat that warms you up.
• Posture, which is the arrangement of your body while sitting or standing, is maintained as a result of muscle contraction.
Types of Muscle Contractions
Skeletal muscle contractions can be categorized as isometric or isotonic.
An isometric contraction occurs when the muscle remains the same length despite building tension. Isometric exercises typically involve maximum contractions of a muscle by using:
• the body’s own muscle (e.g., pressing the palms together in front of the body)
• structural items (e.g., pushing against a door frame)
• contracting a muscle against an opposing force such as a resistance band, or gravity, as shown in Figure 15

Figure 15: Pushing a heavy object involves isometric contractions of muscles in the arms and in the abdomen. This man’s grip on the trolley involves isometric contractions of the hand muscles. The muscles in his legs are contracting isotonically.
An isotonic contraction occurs when tension in the muscle remains constant despite a change in muscle length. Lifting an object off a desk, walking, and running involve isotonic contractions. There are two types of isotonic contractions: concentric and eccentric. In a concentric contraction, the muscle shortens while generating force, such as the shortening of the biceps brachii in your arm when you lift a glass to your mouth to take a drink, or a set of dumbbells, as shown in Figure 16.

Figure 16: An example of an isotonic contraction. The biceps brachii contract concentrically, raising the dumbbells.
During an eccentric contraction, the force opposing the contraction of the muscle is greater than the force that is produced by the muscle. Rather than working to pull a joint in the direction of the muscle contraction, the muscle acts to slow the movement at the joint. Eccentric contractions normally occur as a braking force in opposition to a concentric contraction to protect joints from damage. The muscle lengthens while generating force. Part of training for rapid movements such as pitching during baseball involves reducing eccentric braking which allows greater power to be developed throughout the movement.
Muscles and Exercise
As we learned earlier, your muscles are important for carrying out everyday activities, whether you are picking up a glass of orange juice, walking your dog, or snow wrestling (Figure 17). The ability of your body to carry out your daily activities without getting out of breath, sore, or overly tired is referred to as physical fitness. For example, a person who becomes breathless and tired after climbing a flight of stairs is not physically fit.

Figure 17: You don’t have to be super fit to play in snow, but it might help!
We cannot discuss the effect of exercise on your muscles without first clarifying the confusion between some common terms. It is easy to get confused with the relationship between “physical fitness,” “physical activity,” and “physical exercise.” Some people may think they cannot fit physical activity into their lives because they are unable to afford to join a gym, they do not have the time be involved in an organized sport, or they do not want to lift weights. However, physical activity encompasses so much more than just “working out.” Physical activity is any movement of the body that causes your muscles to contract and your heart rate to increase. Everyday activities such as carrying groceries, vacuuming, walking to class, or climbing a flight of stairs are physical activities.
Being physically active for 60 minutes a day for at least five days a week helps a person to maintain a good level of physical fitness and also helps him or her to decrease their chance of developing diseases such as cardiovascular disease, Type 2 diabetes, and certain forms of cancer. Varying levels of physical activity exist: from a sedentary lifestyle in which there is very little or no physical activity, to high-level athletic training. Most people will find themselves somewhere in the middle of this wide spectrum.
Physical exercise is any activity that maintains or improves physical fitness and overall health. Exercise is often practiced to improve athletic ability or skill. Frequent and regular physical exercise is an important component in the prevention of some lifestyle diseases such as heart disease, cardiovascular disease, Type 2 diabetes and obesity. Regular exercise is also helpful with reduction in, or avoidance of symptoms of depression. Regular exercise improves both muscular strength and endurance. Muscular strength is the ability of the muscle to exert force during a contraction. Muscular endurance is the ability of the muscle to continue to contract over a period of time without getting fatigued. Regular stretching improves flexibility of the joints and helps avoid activity-related injuries.
Effect of Exercise on Muscles
Exercises are generally grouped into three types depending on the overall effect they have on the human body:
• Aerobic, or endurance, exercises, such as cycling, walking, and running, shown in Figure 18, increase muscular endurance.
• Anaerobic exercises, such as weight training, shown in Figure 19, or sprinting increase muscle strength.
• Flexibility exercises, such as stretching, improve the range of motion of muscles and joints.
Aerobic exercise causes several changes in skeletal muscle: mitochondria increase in number, the fibers make more myoglobin, and more capillaries surround the fibers. These changes result in greater resistance to fatigue and more efficient metabolism. Aerobic exercise also benefits cardiac muscle. It results in the heart being able to pump a larger volume of blood with each beat due to an increase in the size of the heart’s ventricles.

Figure 18: Running is a form of aerobic exercise.

Figure 19: This weightlifter shows muscular hypertrophy which he has gained through anaerobic exercise.
Anaerobic, or resistance, exercises cause an increase in muscle mass. Muscles that are trained under anaerobic conditions develop differently giving them greater performance in short duration-high intensity activities. As a result of repeated muscle contractions, muscle fibers develop a larger number of mitochondria and larger energy reserves.
During anaerobic exercise, muscles break down stored creatine phosphate to generate ATP. Creatine phosphate is an important energy store in skeletal muscle. It is broken down to form creatine for the 2 to 7 seconds following intense contractions. After several seconds, further ATP energy is made available to muscles by breaking down the storage molecule glycogen into pyruvate through glycolysis, as it normally does through the aerobic cycle. What differs is that pyruvate, rather than be broken down through the slower but more energy efficient aerobic process, is fermented to lactic acid. Muscle glycogen is restored from blood sugar, which comes from the liver, from digested carbohydrates, or from amino acids which have been turned into glucose.
Two types of muscle fibers make up skeletal muscle:
• Slow twitch muscle fibers, or ”red” muscle, is dense with capillaries and is rich in mitochondria and myoglobin, giving the muscle tissue its characteristic red color. It can carry more oxygen and sustain aerobic activity. The endurance of slow twitch muscles is increased by aerobic training.
• Fast twitch muscle fibers are the fastest type of muscle fibers in humans. These fibers tend to have fewer mitochondria than slow twitch fibers do, but they have larger energy stores. They can contract more quickly and with a greater amount of force than slow-twitch fibers can. Fast twitch fibers can sustain only short, anaerobic bursts of activity before muscle contraction becomes painful. Fast twitch muscle fibers become faster and stronger in response to short, intense activities such as weight training.
Both aerobic and anaerobic exercise also work to increase the mechanical efficiency of the heart by increasing cardiac volume (aerobic exercise), or myocardial thickness (strength training). Anaerobic training results in the thickening of the heart wall to push blood through arteries that are squeezed by increased muscular contractions.
Muscular Hypertrophy
Hypertrophy is the growth in size of muscle fibers and muscles, as shown in Figure 19. Aerobic exercise does not tend to cause hypertrophy even though the activity may go on for several hours. That is why long-distance runners tend to be slim, especially in the upper body. Hypertrophy is instead caused by high-intensity anaerobic exercises such as weight lifting or other exercises that cause the muscles to contract strongly against a resisting force. As a result of repeated muscle contractions, muscle fibers develop a larger number of mitochondria and larger energy reserves. The muscle fibers also develop more myofibrils, and each myofibril contains more actin and myosin filaments. The effect of this activity is hypertrophy of the stimulated muscle.
Factors such as age and sex can also affect muscle hypertrophy. During puberty in males, hypertrophy occurs at an increased rate. In general, males are also able to develop larger muscles because the male body produces far more testosterone than the female body does. On average, an adult human male body produces about eight to ten times more testosterone than an adult female body. Testosterone is an anabolic steroid, which means it increases protein synthesis within muscle fibers, resulting in the buildup of more myosin and actin filaments, and myofibrils. More myofibrils means an increase in strength.
Athletic heart syndrome is hypertrophy of cardiac muscle in response to exercise. A larger heart is able to pump more blood with a single beat, resulting in a lower resting pulse rate than average. The average resting heart rate for a healthy adult is between 60 and 100 beats per minute, but an athlete can have a resting pulse rate of 40 beats per minute or less! These changes would indicate heart-disease if observed in a person who is not active, but in an athlete a large heart with a slow resting pulse is the result of normal and healthy muscle growth, and indicates a high level of fitness.
Proper rest and recovery are also as important to health as exercise, otherwise the body is in a permanently injured state and will not improve or adapt well to the exercise. Therefore, it is important to remember to allow adequate recovery time of muscles between exercise sessions. This type of rest is called active rest.
Muscle Atrophy
To remain healthy, muscles must be used. The condition in which muscle mass is lost is called atrophy. Atrophy can occur if muscles do not get enough exercise, or if an injury such as bone fracture causes immobility. Atrophy is the reverse of hypertrophy, muscle fibers become smaller, which causes the muscle to become smaller. Atrophy can also result from a spinal injury (CNS damage) leading to muscle paralysis, which the athlete in Figure 20 experiences. Diseases such as muscular dystrophy, amyotrophic lateral sclerosis (ALS, or Lou Gehrig’s disease), and polio also cause muscle atrophy.

Figure 20: Muscular paralysis and the resulting atrophy of the leg muscles, as this marathon racer with paraplegia has experienced, does not have to prevent a person from developing aerobic fitness.
Homeostatic Imbalances of the Muscular System
Hypertrophy of internal organs can sometimes be harmful. For example, hypertrophic cardiomyopathy, or HCM, is a disease of the heart muscle in which a portion of the cardiac muscle (usually the left ventricle) is enlarged without any obvious cause. HCM has been related to the sudden death of young athletes, but it is also of significance as a cause of sudden unexpected cardiac death in any age group and as a cause of disabling cardiac symptoms. Most patients’ symptoms may be managed medically without needing surgery. HCM is not to be confused with athletic heart syndrome which is hypertrophy of the heart muscle in response to exercise.
Delayed Onset Muscle Soreness (DOMS) is the pain or discomfort often felt 24 to 72 hours after exercising and generally goes away within 2 to 3 days. Once thought to be caused by lactic acid buildup, a more recent hypothesis is that it is caused by tiny tears in the muscle fibers caused by eccentric contraction, or an increased level of training. Since lactic acid is quickly taken away by in the blood, it cannot explain the pain experienced days after exercise. Delayed onset muscle soreness can occur after any kind of exercise, particularly if the body is unconditioned for that exercise.
Tendinitis is a painful disorder of a tendon. Generally tendinitis is referred to by the body part involved, such as Achilles tendinitis which affects the Achilles tendon, shown in Figure 21, or patellar tendinitis (jumper’s knee, which affects the patellar tendon). It was believed that tendinitis was due to inflammation of a tendon, although this is now being questioned. Chronic overuse of tendons leads to microscopic tears within the collagen matrix, which gradually weakens the tissue. Eccentric muscle contractions are being researched for their ability to speed rehab of weak or injured tendons. Achilles tendinitis has been shown to benefit from high load eccentric contractions.

Figure 21: The Achilles tendon is a large tendon connecting the heel to the muscles of the calf.
Neuromuscular diseases are those that affect the muscles and/or their nervous control. In general, problems with nervous control can cause spasticity or paralysis, depending on the location and nature of the problem. A large number of neurological disorders leads to problems with movement, ranging from strokes and Parkinson’s disease, to the very rare and incurable degenerative disorder, Creutzfeldt-Jakob disease.
Diseases of the motor end plate include myasthenia gravis, a form of muscle weakness due to antibodies to the acetylcholine receptor. Tetanus and botulism are bacterial intoxications in which bacterial toxins cause muscular spasms by blocking the action of inhibitory neurotransmitters (tetanus) or decreased muscle tone (botulism).
Myopathies are diseases affecting the muscle itself, rather than its nervous control. Muscular dystrophy is a large group of diseases which leads to progressive loss of muscle strength and decreased life span.
Smooth muscle plays a role in a large number of diseases affecting blood vessels, the respiratory tract (asthma), the digestive system (irritable bowel syndrome), and the urinary tract (urinary incontinence). However, these diseases are not usually confined just to the muscular tissue, and affect other tissues too.
Images courtesy of:
http://www.flickr.com/photos/bjornb/60128667/. CC-BY-SA.
Louisa Howard. http://commons.wikimedia.org/wiki/Image:Human_skeletal_muscle_tissue_1_-_TEM.jpg. Public Domain.
http://en.wikipedia.org/wiki/Image:Human_Aortic_SMC.jpg. CC-BY-SA.
Dr. S. Girod. http://en.wikipedia.org/wiki/Image:Glanzstreifen.jpg. CC-BY-SA.
http://commons.wikimedia.org/wiki/Image:Skeletal_muscle_-_longitudinal_section.jpg. Public Domain, GFDL.
USFG. http://commons.wikimedia.org/wiki/File:Illu_upper_extremity.jpg. Public Domain.
http://commons.wikimedia.org/wiki/Image:Arm_flex_supinate.jpg
http://commons.wikimedia.org/wiki/Image:Triceps_brachii.png. GNU-FDL, CC-BY-SA.
http://commons.wikimedia.org/wiki/Image:Skeletal_muscle.jpg. CC-BY-SA.
Slashme. http://en.wikipedia.org/wiki/File:Sarcomere.svg. GNU-FDL.
Utilisateur:Dake. http://commons.wikimedia.org/wiki/Image:Synapse_diag3.png,
http://commons.wikimedia.org/wiki/Image:Synapse_diag4.png. CC-BY-SA, GNU-FDL.
http://en.wikipedia.org/wiki/Image:Querbr%C3%BCckenzyklus_2.png
http://en.wikipedia.org/wiki/Image:Querbr%C3%BCckenzyklus_3.png
http://en.wikipedia.org/wiki/Image:Querbr%C3%BCckenzyklus_4.png
http://commons.wikimedia.org/wiki/Image:ATP_symbol.svg. CC-BY-SA.
Snowdog. http://commons.wikimedia.org/wiki/Image:Street-defibrillator.jpg. Public Domain.
http://commons.wikimedia.org/wiki/Image:Small-Intestine-highlighted.gif. Public Domain.
Zoom Zoom. http://www.flickr.com/photos/zoomzoom/304130574/. CC-BY-SA.
George Stepanek. http://commons.wikimedia.org/wiki/File:PreacherBenchBicepsCurl.JPG. CC-BY-SA.
ZeWrestler. http://commons.wikimedia.org/wiki/Image:Snowball_fight_MSU.jpg. Public Domain.
Cpl. Benjamin Cossel. http://en.wikipedia.org/wiki/Image:Weightlifting.jpg. Public Domain.
Euthman. http://www.flickr.com/photos/euthman/357322273/. CC-BY-SA- 2.0.
http://commons.wikimedia.org/wiki/File:Achilles-tendon.jpg. Public Domain.